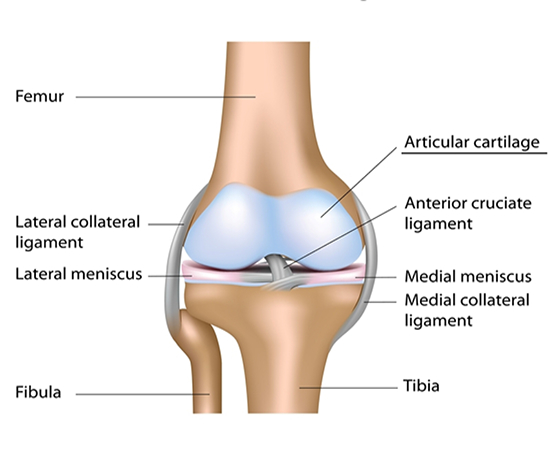
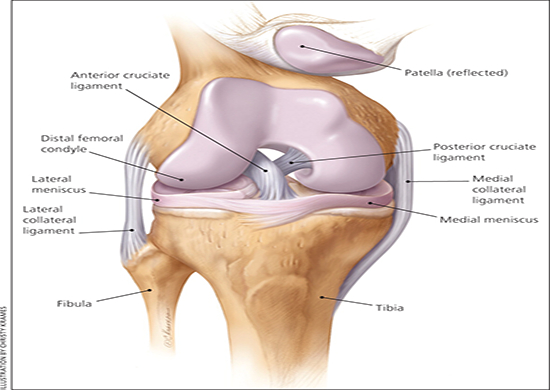
There are two forms of cartilage in the knee. One is a surface, or “articular” cartilage, which is the white, glistening cartilage on the surface of the bone. This is very smooth and designed to glide
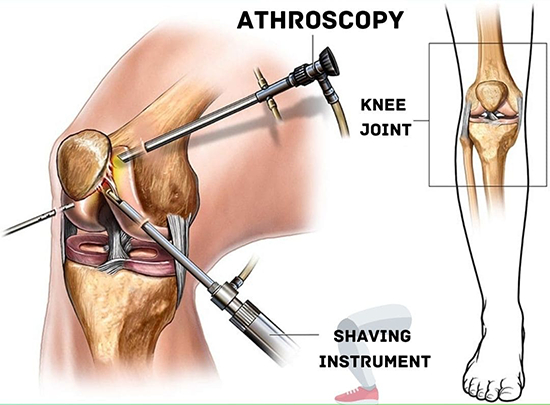
without any friction. The second type of cartilage is the “meniscus” cartilage. This is more of a “bumper cushion” cartilage, which sits between the thigh and shin bones, providing a shock-absorbing effect during athletics. When the knee is violently twisted or other injuries occur, the meniscus cartilage can be torn. If this is a small tear and does not have much in the way of symptoms, it can be treated without surgery. If it is a large tear, with a loose fragment that flips up into the joint and blocks or limits motion, surgery is indicated. The advance of arthroscopic surgery has made removal or repair of these tears much easier, and is associated with very little in the way of surgical trauma. Patients can recover quite quickly and be back to sports within a matter of days or weeks.
If injury occurs to the articular cartilage of the knee, treatment can be more problematic. There is no widely used, well proven way to regenerate surface cartilage of significant damage has occurred. However, treatment with activity modification, anti-inflammatory medications, occasionally cortisone injections, and a variety of developing arthroscopic surgical techniques is useful in the majority of patients.